How LLM-Based Extraction Turns Unstructured Orders into Workflow-Ready Data in Radiology and Across Healthcare
Healthcare has spent decades digitizing documents: scanning, indexing, storing, retrieving. But digitization by itself doesn’t make anything faster. It moves paper into pixels. The information is technically accessible, but it still doesn’t move.
The shift that matters is when documents stop merely being things to file and start becoming inputs to action — when unstructured clinical paperwork becomes structured enough to route work, trigger notifications, and push patient information into systems of record without a staff member manually shepherding every step.
Radiology is one of the clearest places to see what that shift looks like in practice. Not because radiology is uniquely burdened with paperwork (it isn’t), but because the pain is unusually measurable. Schedules, scanners, and staffing all create hard constraints, and those constraints carry real cost. When intake is slow or ambiguous, equipment sits idle, staff burn time chasing information, and patients wait. When intake is structured and routable, throughput improves, utilization goes up, and the downstream chain gets easier almost by default.
Radiology Orders Are a Stress Test for Healthcare Operations
Imaging centers and radiology departments receive orders in formats that vary widely across referring providers, often unstructured (scanned, faxed, emailed, or portal-exported), packed with critical details buried in narrative text, and tied to real downstream dependencies like scheduling, prior authorization, billing, and routing.
This is exactly where traditional extraction approaches tend to break down. The fields that matter most aren’t always printed cleanly, consistently, or in predictable positions. They’re abbreviated, phrased differently, implied, or embedded in free text.
The information exists. It just doesn’t move on its own.
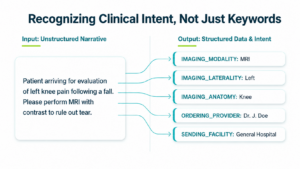
LLMs change this because they can recognize clinical intent within that messy middle — provided you deploy them with bounded goals, workflow context, and operational governance. This isn’t about “AI doing radiology.” It’s about AI handling the paperwork that slows radiology down.
What We Extract Today and What It Unlocks
We built LLM-based clinical extraction for radiology to move beyond document recognition and indexing toward workflow-ready intelligence and power real imaging operations.
As part of our first LLM-powered enhancement to the Extraction module, we implemented entity identification for:
- IMAGING_MODALITY
- IMAGING_LATERALITY
- IMAGING_ANATOMY
- ORDERING_PROVIDER_NAME
- ORDERING_PROVIDER_ADDRESS
- SENDING_FACILITY_NAME
Radiology LLM Entities: More Usable Order Data, Earlier in the Workflow
Concord’s new radiology-specific LLM entities, including Modality, Laterality, and Anatomy, help teams identify order details earlier so documents can be tagged, routed, and prioritized more efficiently. That visibility helps teams move orders into the right workflow sooner.
A walk-in X-ray may not require the same process as a CT or MRI that needs scheduling and authorization, while PET studies may require specialized planning and time-sensitive resources. When modality data and workflow tags are available earlier, staff can more quickly find orders that match open appointment slots, help protect revenue by filling canceled appointment times, and keep scheduling, intake, and prior authorization teams aligned.
If your team needs specific fields extracted from radiology orders — or from another high-volume workflow — contact us. Concord can work with you to identify the data that matters most and improve how information is routed, reviewed, and acted on.
Why the LLM Approach Matters Operationally
What LLMs change isn’t just which entities can be extracted, it’s how quickly new, high-value entities and workflows can be deployed.
Historically, adding new extraction logic meant template work, model retraining, brittle rules, and long validation cycles. With LLMs, we can iterate faster and introduce new workflow-driving signals without rebuilding the foundation each time. So, when operations teams identify friction such as a missing referral attribute, an authorization requirement, or a specialty routing rule, we’re no longer constrained to static field libraries.
In healthcare operations, extracted fields aren’t metadata. They represent decisions that need to happen, and LLMs make those decisions programmable.
Clinical Fields Drive Operational Decisions
Radiology makes the relationship between data and decisions particularly concrete:
- Modality affects equipment availability, protocols, staffing, and scheduling constraints. It also reveals complexity that isn’t obvious at first glance — a single incoming document may contain orders for multiple modalities (say, a chest X-ray, a chest CT, and an ultrasound), each requiring a completely different operational path. Without modality parsing, staff may not realize they’re looking at three separate workflows until they’re already partway through one of them.
- Anatomy affects exam type, prep requirements, duration, and sometimes which department or facility can perform the study.
- Laterality affects site specificity — which side, unilateral vs. bilateral, and how the order should be interpreted operationally.


When these details are incomplete or inconsistent, someone must stop what they’re doing and go play detective — calling back, cross-referencing, clarifying. That detective work is what delays care. LLM extraction turns those embedded signals into structured, usable inputs that can drive workflows before someone has to pick up the phone.
Straight-Through Processing: The Operational North Star
If there’s a single concept that explains why this matters, it’s Straight-Through Processing (STP).
In the context of healthcare, STP means receiving documents and data, extracting what’s needed, matching it to the right context, and moving it into the system of record with minimal manual handling. It doesn’t mean removing humans from the process. It means reducing unnecessary touches: less re-keying, less queue triage, fewer misroutes, fewer escalations, and fewer “who owns this?” loops.
The biggest unlock for STP is pairing clinical fields with patient identifiers: name, date of birth, patient ID / MRN. When identifiers are extracted reliably, documents can be matched to the right chart and processed into the EHR or other system of record without manual searching and attachment gymnastics.
That’s the point where extraction stops feeling like a feature and starts feeling like time returning to the business.

What These Fields Enable in Real Radiology Work
Scheduling: From Reactive to Proactive
Radiology scheduling isn’t just “find a time.” It’s matching the right patient to the right machine, protocol, and team. When modality, anatomy, and site specificity are structured at intake, orders route to the right scheduling pool immediately, staff can validate readiness faster, and exceptions surface earlier — before the schedule takes the hit.
But structured data doesn’t just improve how orders flow into the schedule. It also changes how teams manage the schedule itself.
When openings appear, whether from cancellations, no-shows, or shifting priorities — staff can search queued orders by modality to find studies that fit available slots, rather than manually combing through a backlog hoping to find a match. Teams can identify high-priority patients earlier and hold appropriate scheduling windows before those slots fill up.
The result is fewer clarification calls, fewer reschedules, and fewer downstream surprises — along with better utilization of the equipment and staff time that represent some of radiology’s largest fixed costs.
Protecting Revenue When the Schedule Breaks
Cancellations are a fact of life in radiology. But for certain modalities, a cancellation doesn’t just mean an open slot, it means direct cost exposure.
PET studies are a clear example. They require radioactive isotopes that must be ordered in advance and have limited half-lives. A canceled PET appointment doesn’t just leave a scanner idle — it can mean wasted material that can’t be recovered. The faster a team can identify a replacement patient and fill that slot, the more of that investment they protect.
When PET orders (and other high-cost modalities) are tagged and sitting in filterable queues, rescheduling becomes a search problem rather than a scramble. Staff know exactly which studies are pending, can match them to open windows, and can move quickly enough to salvage time-sensitive resources.
This is where the connection between extraction and revenue becomes concrete: structured data doesn’t just save time, it protects the operational economics of running an imaging department.
Routing to the Right Team
A huge portion of operational drag in healthcare isn’t complexity, it’s misdirection. When provider, facility, and imaging details are structured, work can route by service line, modality, or sending facility. The right staff get notified without broadcast noise, and queues stop functioning as inboxes and start functioning as workflows.
In practice, this means scheduling staff who handle specific modalities can work from dedicated queues rather than sorting through a shared pool of everything. Work is centralized by relevance, more people get faster access to the orders they actually need to act on, and less time is spent simply locating the right document.
Routing isn’t glamorous, but it’s one of the highest-leverage time savers in healthcare administration.
Faster Authorization Readiness
Radiology lives alongside constant prior authorization pressure and many prior auth teams work remotely, which makes visibility even more critical.
Structured imaging details make it easier to detect missing information earlier, standardize what gets packaged for submission, and reduce rework loops caused by incomplete or mismatched order details. When workflow status is visible and tagged, distributed teams can see where each order stands — what’s been started, what’s complete, who’s working on what — without duplicating effort or waiting on status updates.
Even when authorization isn’t fully automated, reducing documentation churn and giving remote staff clear, immediate access to the information they need is a significant operational win.
Cross-Department Visibility and Standardized Workflows
Radiology departments don’t operate in isolation. Orders, records requests, legal inquiries, and clinical correspondence all flow through overlapping teams — often across multiple sites. When each department relies on its own process for tracking what’s come in and where it stands, work gets duplicated, things fall through cracks, and no one has a reliable picture of overall status.
When incoming documents are parsed, tagged, and tracked within a shared workflow — with clear status indicators visible to everyone who needs them — each department can operate from a standardized process. Scheduling knows what’s been ordered. Prior auth knows what’s in progress. Medical records can locate what’s been requested. Teams aren’t re-sorting the same information or wondering whether someone else already handled it.
That kind of visibility also helps teams meet internal SLAs and reduces the coordination overhead that comes with managing high-volume inbound workflows across distributed staff.
Findability in Shared Workspaces
“Where is the order?” sounds like a small question until you multiply it across teams, sites, and days. When extracted entities become searchable filters, staff can find documents without knowing filenames, teams can locate orders by provider, modality, facility, or anatomy, and shared workspaces become operational systems rather than storage closets.
The ability to surface relevant data points on screen immediately — rather than opening, reading, and mentally cataloging each document — changes how quickly staff can act. In distributed healthcare operations, findability is throughput.
Not sure where extraction could make the biggest impact?
Concord can help your team assess high-volume intake workflows, identify the data points that drive routing and scheduling decisions, and determine where LLM-based extraction could reduce manual work, improve visibility, and help teams act sooner.
Request a workflow assessment
Faster Processing, Better Patient Experience
Most of the operational benefits above are framed in terms of staff efficiency and cost, but they also have a direct downstream effect on patients.
When orders are processed faster, patients hear back sooner. They get scheduled sooner. And when studies are completed, results reach referring clinicians faster. That turnaround time affects not just patient experience, but referral satisfaction — which, for imaging centers that depend on a steady flow of orders from referring providers, is a business outcome as much as a clinical one.
Reducing the time between “order received” and “patient contacted” is one of the most tangible ways that structured intake translates into better care delivery.
Why Radiology Is the Proving Ground — and How This Expands
Radiology works as a proving ground because it’s hard in the right ways: the inputs are messy, the downstream workflows are tightly constrained, delays are visible immediately, and outcomes are measurable. It’s one of the few areas in healthcare where administrative friction shows up directly in operational metrics — idle scanners, backlogged schedules, longer patient wait times, and wasted resources.
One radiology customer using Concord’s LLM extraction saw meaningful improvements across several of these dimensions — more seamless order processing, better schedule utilization, reduced manual effort in routing and triage, and improved coordination across distributed teams. The extraction capabilities didn’t replace their staff; they removed the repetitive sorting, searching, and re-keying that kept staff from doing higher-value work.
If you can reliably extract clinical intent from imaging orders, the same pattern applies across the broader administrative landscape of healthcare:
- Referrals
- Prior authorizations
- Lab orders and results
- Specialty intake
- Claims and billing documentation
- Clinical correspondence and care coordination
The underlying logic is consistent: if you can extract the signals that move work, you can automate the movement of work. That’s why we treat radiology extraction as a starting line, not a finish line.
The How: LLMs Plus Workflow Context
Extraction doesn’t create value in isolation. It creates value when it’s connected to reliable intake (multi-channel, multi-format), a shared workspace where documents, people, and processes converge, workflow rules that turn extracted fields into routing, notifications, and validation, and integrations that move data into systems of record.
The practical architecture is straightforward: documents arrive, key signals are extracted, the right work is triggered, and the right system is updated. That’s how clinical extraction becomes workflow intelligence.
A Practical Perspective: Build Workflows That Matter, Then Expand
A lot of healthcare AI initiatives fail because they try to solve everything at once. The practical path is more methodical:
- Identify where workflow friction is measurable.
- Extract the signals that unblock that workflow.
- Connect those signals to routing, notifications, validation, or integration.
- Measure the impact.
- Expand from there.
LLMs accelerate this cycle. They reduce the gap between “we see a bottleneck” and “we deployed a workflow that addresses it.” Instead of waiting on long model retraining or rigid template configuration, operations teams can evolve their automation layer as new patterns emerge.
The real value isn’t just better extraction accuracy — it’s faster workflow deployment tied directly to operational outcomes.
Ready to make clinical intake more actionable?
If your team needs specific fields extracted from radiology orders, referrals, prior authorization documents, or another high-volume workflow, contact Concord to discuss what data matters most and how it could be used to route, prioritize, review, and act on information faster.